Consolidate primary healthcare resources
Public healthcare resources should be allocated to cater to the healthcare needs for all in a sustainable manner. As illustrated above, there will be a need to increase public expenditure on primary healthcare (PHC) services as an investment so as to achieve the target of reallocation of public health resources to achieve a sustainable health system. A focus on chronic disease prevention and management is widely established as one of the most cost-effective ways to envisage sustainability of the healthcare system. With the investment, it is expected that there will be an increase in the overall health expenditure in PHC from both the public and private sectors. The additional resources required would have to be drawn either through reallocation from existing resources or injection of new ones.
To improve accessibility to quality PHC for the general public and redress the imbalance between the public and private healthcare sectors, strategically the Government strives to optimise the utilisation of private healthcare resources and leverage on the private sector’s capacity for providing PHC services, with a view to relieving pressure on the public sector and thereby enhancing the sustainability of the healthcare system. As recommended in the “Your Health Your Life” Healthcare Reform Consultation Document in 2008, to pursue PPP in healthcare in Hong Kong to subsidise the community to make better use of resources in the private sector for delivering service for public sector patients, thus allowing the public healthcare system to continue to serve as an essential safety net for the population and be accessible to those who lack the means to pay, we have recommended that PHC services should be purchased from the private sector and patients should be partially subsidised to undertake preventive care in the private sector [19]. In this connection, the Government proposes to improve the existing financing schemes, with various forms of subsidisation and PPP through strategic purchasing, to enhance the accessibility and affordability of PHC services in the community.
Public Health Expenditure
Figure 4.1:
The distribution of PHC expenditure in Public Health Expenditure
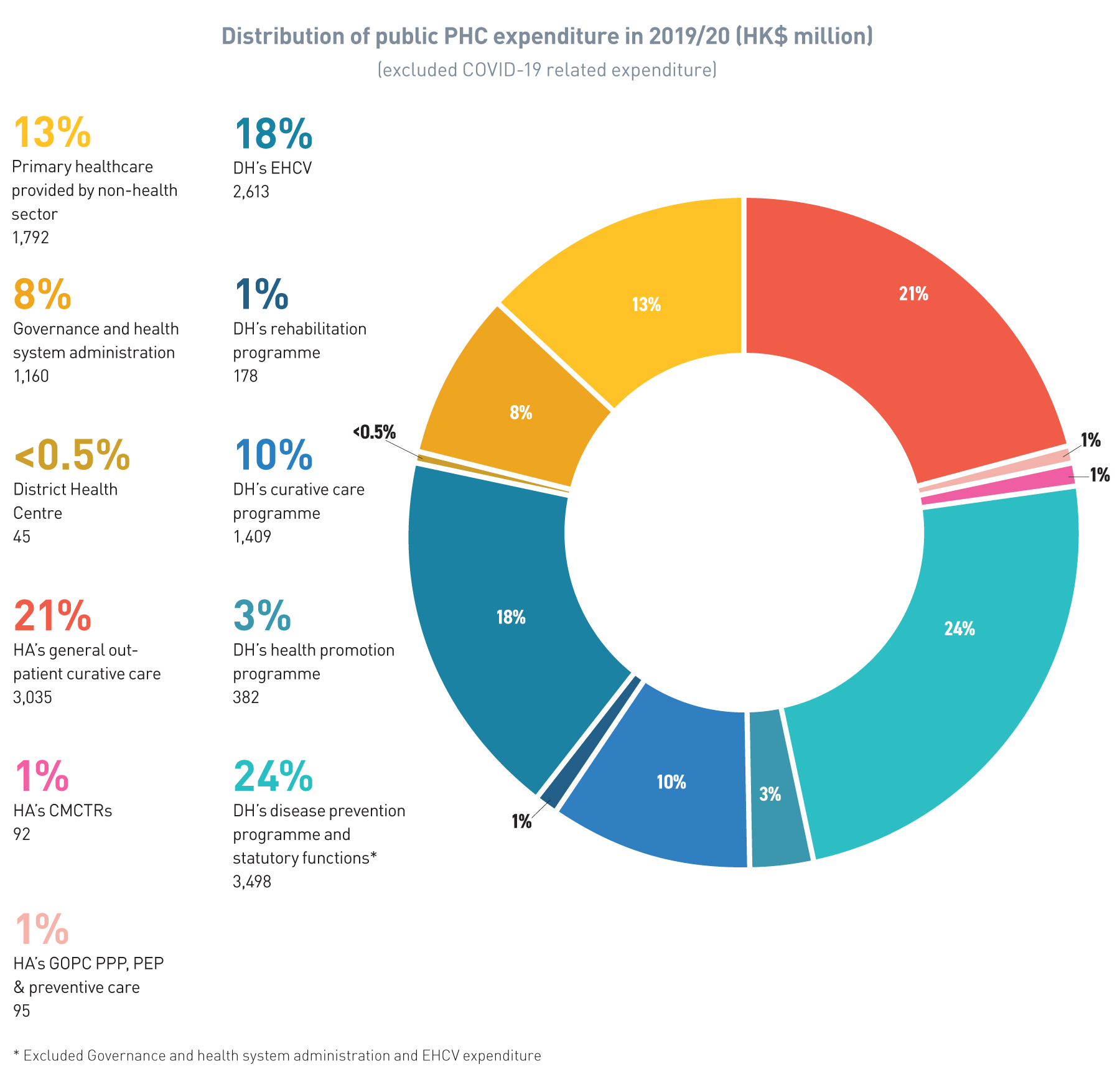
Source: DHA[7]
Private Health Expenditure
6 While the Government does not have full grasp of the total private health expenditure on PHC in the market due to difficulty in differentiating PHC from other secondary out-patient services in the private sector, we have taken the assumption that 50% of out-patient curative care and 50% of administration of health financing are classified as PHC services in the private sector.
Figure 4.2:
Estimated PHC expenditure in the public and private sectors (in HK$ million) and the proportion of PHC expenditure as a % of GDP
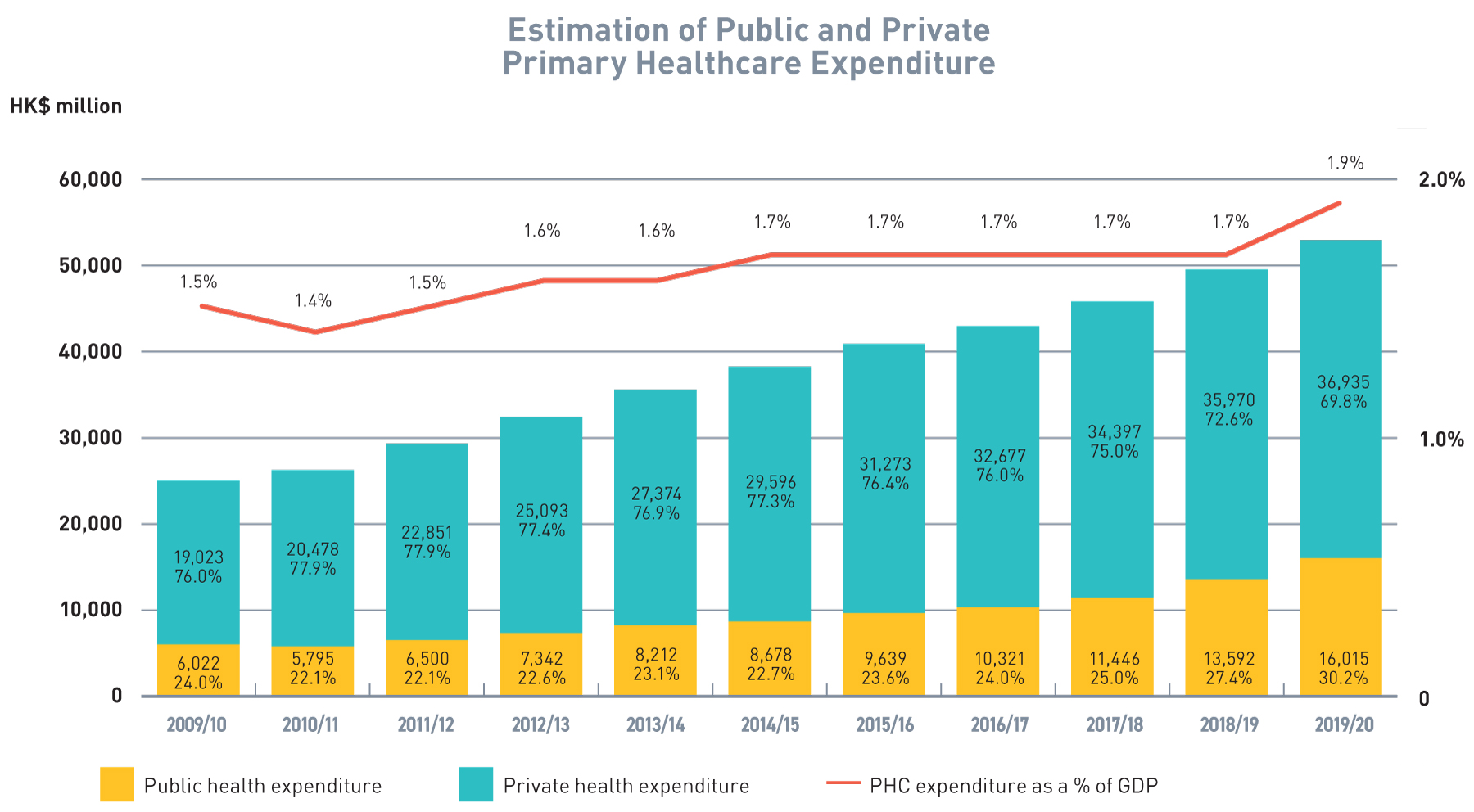
Source: DHA
The situation is different for secondary and tertiary care where the public sector is the major provider of services with private expenditure accounting for only 37% (Figure 4.3) or $47,415 million. Given the limited supply of services in private secondary and tertiary care, there would be limited scope for the Government to achieve savings in secondary and tertiary care, which are curative in nature, through PPP.
Figure 4.3:
Composition of Current Health Expenditure (in HK$ million), 2019/20
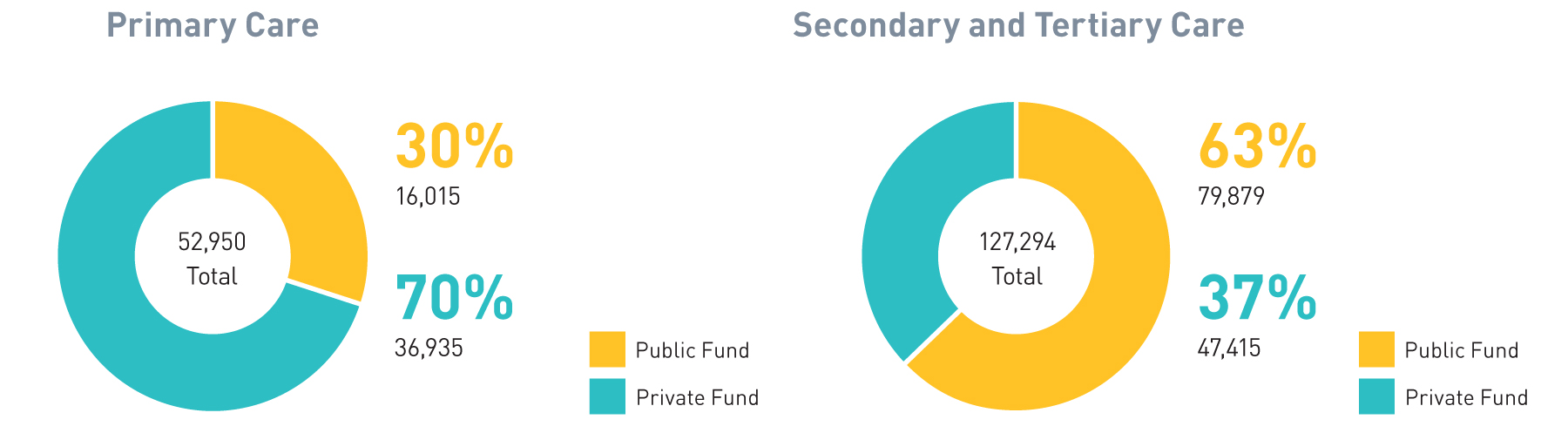
Source: DHA
Public-private partnership
Table 4.1
Key Examples of Public-private Partnership Schemes in Primary Healthcare
![]()
Department of Health
![]()
Health Bureau
![]()
Hospital Authority
There is an increasing participation of private service providers in public PHC (Figure 4.4) that among the public expenditure on PHC, the share paid to private service providers has been increasing steadily over the past decade from only 8% in 2010/11 to about 28% (excluding COVID-19 related expenditure) in 2019/20.
Figure 4.4 :
Public health expenditure on PHC by public service providers and private service providers
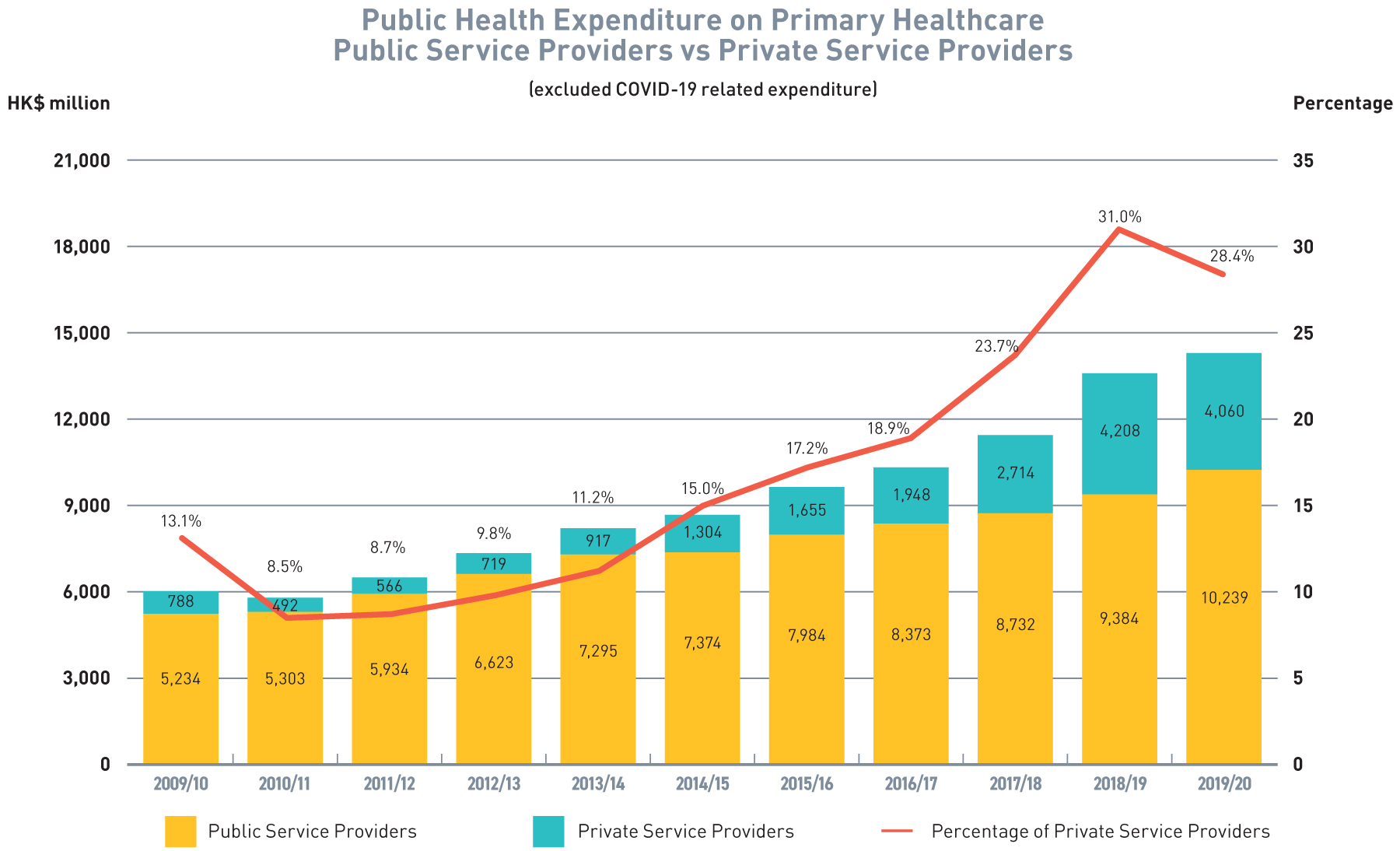
Source: DHA
The Challenges
Our Aim
Recommendation 4.1
Subsidisation for chronic disease screening and management
Recommendation 4.2
Reallocation of primary healthcare resources – the Elderly Health Care Voucher
Recommendation 4.3
Reallocation of primary healthcare resources – strategic purchasing of primary healthcare services
Table 4.3
Scope of Service of Strategic Purchasing Office(SPO)
Population-wide Programmes
- Population-wide Programmes are programmes that are designed on population-wide basis under defined scope of target providers and clients, aiming to achieve the Government’s healthcare policies and objectives.
- SPO will explore, plan, launch, administer, review and evaluate the programmes according to the programme policy objectives
- Partnership and synergy with DHCs under the Health Bureau and the CMCTRs would be
planned - In view of the fact that the resources of Hong Kong's CM sector are mainly concentrated in the private market, we will also explore enhancing CM PHC services by, inter alia, resource allocation through strategic purchasing.
HA Patient Programmes
- HA Patient Programmes are programmes that would cover HA patients only, aiming to achieve the Government’s objective of building an integrated healthcare system with respect to HA services.
- All existing HA PPP programmes will migrate to SPO by phases for management and administration
Elderly Health Care Voucher (EHCV) Scheme
- EHCV Scheme will migrate to SPO for management and administration
- SPO will leverage on the EHCV Scheme and other available financial resources to build incentives in the SPPs with a view to develop desirable health seeking and health providing behaviour toward targeted health outcomes for the population